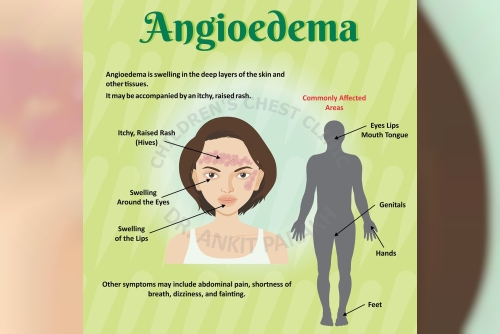
Angioedema is localized swelling of the deeper layers of the skin and mucous membranes (i.e., the subcutaneous tissue and submucosa), often occurring in areas such as the lips, eyelids, tongue, face, hands, genitalia, or airway.
Unlike urticaria (hives), which principally involves more superficial swelling and is often raised and itchy, angioedema is deeper and may not involve surface itching or reddening. However, angioedema can occur simultaneously with urticaria in many cases.
Swelling from angioedema usually develops rapidly (minutes to hours) and often resolves spontaneously over a few hours to days but in severe cases, especially when the airway is involved, it may be life-threatening.
There are broadly two mechanistic classifications of angioedema
Histamine or mast cell mediated angioedema (often linked with allergic reactions)Bradykinin mediated angioedema (often independent of classic allergy pathways)Each class has different triggers, clinical features, and treatment implications.Causes and Triggers of AngioedemaAngioedema can result from many causes. Some are common and benign; others are rare but dangerous. Below is a categorization of the major types and triggers.
1. Allergic (histaminergic) angioedemaThis is the classic form, associated with an immediate hypersensitivity (type I) reaction. Mast cells or basophils release histamine, leukotrienes, and other inflammatory mediators, increasing vascular permeability and causing swelling.
Common triggers include:
Foods: peanuts, tree nuts, fish, shellfish, eggs, milk, etc.
Medications: penicillins, nonsteroidal anti-inflammatory drugs (NSAIDs), aspirin, certain antibiotics, or others to which one has hypersensitivity
Insect stings or bites
Latex or contrast agents (e.g. radiographic dye)
Environmental factors: temperature changes, sunlight, cold exposure, or mechanical stimuli (pressure, friction) may exacerbate in susceptible individuals
In many allergic cases, urticaria (hives) is present concomitantly, which helps in diagnosis.
2. Drug-induced & nonallergic formsSome medications can cause angioedema not through IgE allergy but via other biochemical pathways (often involving bradykinin). The most famous class is ACE (angiotensin-converting enzyme) inhibitors. Because ACE also helps break down bradykinin, blocking ACE can lead to increased bradykinin levels and swelling.
This form typically lacks hives and can occur even after months or years of therapy.
Other drugs implicated include ARBs (angiotensin receptor blockers), neprilysin inhibitors, and certain chemotherapeutic or immunologic agents.
3. Hereditary Angioedema (HAE)A rare, genetic form, usually autosomal dominant, due to deficiency or dysfunction of C1 esterase inhibitor (C1-INH). This leads to uncontrolled activation of the complement and contact (kallikrein–bradykinin) systems, resulting in excessive bradykinin and vascular leakage.
Attacks may be spontaneous or triggered by minor trauma, stress, dental procedures, hormonal changes, or infection.
4. Acquired C1-INH deficiency (Acquired angioedema, AAE)Less common than hereditary type, this occurs when C1-INH is consumed or neutralized due to another disease (e.g. lymphoproliferative disorders, autoimmune disease) rather than a congenital defect.
5. Idiopathic angioedemaIn many patients, no clear trigger or cause is found. The condition may be chronic and recurrent. It may have features of either histaminergic or non-histaminergic pathways.
Often, workup is done to exclude allergic, drug-induced or hereditary causes.
Pathophysiology (Mechanisms)Histaminergic (mast cell–driven): Allergen or trigger leads to cross-linking of IgE on mast cells, degranulation and release of histamine, leukotrienes, and prostaglandins. These mediators increase vascular permeability (capillaries leak plasma into the tissue), causing swelling.
Bradykinin-mediated (C1-INH deficiency or ACE inhibitor–associated): In these, increased generation or reduced degradation of bradykinin (a potent vasodilator and permeability mediator) is central. Bradykinin increases vascular permeability without involvement of histamine.
Because of these mechanistic differences, histaminergic angioedema often responds to antihistamines, corticosteroids, and epinephrine, whereas bradykinin-mediated forms do not reliably respond to them.
Clinical Features and DiagnosisPresentation & SymptomsRapid swelling in the affected area, often non-pitting, non-pruritic (i.e. not very itchy)
May have pain or burning sensation rather than itching in some cases
If airway (larynx, tongue) is involved: voice changes, stridor, difficulty breathing, hoarseness — this is an emergency
Gastrointestinal angioedema (intestinal swelling) can cause abdominal pain, vomiting, diarrhea, nausea
Often resolves in hours to days if not life-threatening
Diagnostic EvaluationClinical history and physical exam
Timing, triggers, recurrence, drug history (especially ACE inhibitors), family history
Presence or absence of urticaria
Laboratory/complement testing (especially if hereditary or acquired forms suspected)
C4 complement level (often low during attack)
C1 esterase inhibitor (functional and antigenic)
C1q levels (in acquired forms)
Autoimmune or lymphoproliferative workup in acquired cases
Genetic testing in hereditary forms if needed
Allergy testing, if allergic cause suspected (skin prick tests, specific IgE)
Imaging or endoscopy, if internal or airway involvement is suspected
Provocation or challenge tests (rarely) under controlled settings
Distinguishing histaminergic vs bradykinin-mediated forms is key, because their treatments differ substantially.
Treatment of AngioedemaTreatment depends on severity, airway involvement risk, and underlying mechanism (histamine- vs bradykinin-mediated).
Immediate and supportive measuresAirway protection: In swelling of tongue, throat or voice change, securing the airway (intubation or tracheostomy, if needed) is top priority.
Stop offending agent or trigger: Discontinue suspected medications (e.g. ACE inhibitors) immediately.
Observation and monitoring, especially in moderate cases
Histamine-mediated angioedema (allergic type)Since this is mediated via mast cell degranulation:
Antihistamines (H1 antagonists) are first-line therapy. Second-generation non-sedating antihistamines (e.g. cetirizine, loratadine, desloratadine, fexofenadine, levocetirizine) are commonly used.
In more severe cases, H2 blockers (e.g. ranitidine, famotidine) may be used as adjuncts
Corticosteroids (oral or systemic) may reduce inflammation and swelling, particularly in moderate to severe cases.
Epinephrine (intramuscular) is indicated if there is impending anaphylaxis or airway compromise.
Adjunctive therapies (e.g. leukotriene receptor antagonists) sometimes used in refractory cases.
Most mild to moderate cases resolve with this regimen; however, careful follow-up is needed.
Bradykinin-mediated angioedema (hereditary, ACE-inhibitor, acquired)Because the pathophysiology is different, standard allergy-based therapies are often ineffective. Treatment is more specialized:
Acute attack managementC1 esterase inhibitor (C1-INH) concentrate (plasma-derived or recombinant) is a mainstay in hereditary and some acquired forms.
Icatibant, a bradykinin B2 receptor antagonist (subcutaneous injection) can rapidly relieve symptoms.
Ecallantide (plasma kallikrein inhibitor) is another option (in some regions) for HAE.
Fresh frozen plasma (FFP) may be used as a source of C1-INH in settings where more specific agents are unavailable (but carries risks)
Supportive care (fluids, analgesia, airway monitoring)
Prophylaxis and long-term preventionAttenuated androgens (e.g. danazol) historically used to raise C1-INH levels in hereditary cases
Antifibrinolytic agents such as tranexamic acid (less effective)
Prophylactic C1-INH therapy in people with frequent severe attacks
Newer therapies: agents targeting kallikrein, complement, or bradykinin pathways (ongoing research)
In cases of ACE inhibitor–induced angioedema, the offending drug must be discontinued permanently.
Special and emergency considerationsIn airway-compromising swelling, intubation or even emergency surgical airway may be necessary.
Even for milder cases, observation in a controlled environment is prudent until swelling subsides.
Patient education on avoidance of known triggers, early recognition, and carrying emergency epinephrine (if allergic component) is essential.
Prognosis & PreventionMany mild angioedema episodes resolve spontaneously or with therapy within 24 to 72 hours.
Recurrence is common, especially in hereditary, acquired, or idiopathic forms.
The presence of airway involvement is the greatest risk factor for morbidity and mortality.
Preventive strategies include avoiding known triggers, being cautious with medications associated with angioedema, and in high-risk cases, prophylactic therapy under specialist care.
Cephalexin Capsules Distributors (Why Mentioned & Relevance)I include below a short note about cephalexin capsules distributors, since you asked to include that keyword in the content.
Cephalexin is a widely used oral cephalosporin antibiotic (often in capsule form) for treating bacterial infections (e.g. respiratory, urinary tract, skin).
In India (and elsewhere), there are many manufacturers, suppliers, and distributors of cephalexin capsules. For example, suppliers in Delhi are listed via trade directories as cephalexin distributors, such as Elikem Pharmaceuticals Pvt Ltd., Syncom Formulations India Ltd., and others.
Additionally, platforms like PharmaCompass list cephalexin API (active pharmaceutical ingredient) manufacturers, exporters, and distributors that supply to finished formulation makers.
If you are interested, I can help you with a listing of cephalexin capsules distributors in a particular region (e.g. Gujarat or Surat) along with contact details.
Summary & Key TakeawaysDefinition: Angioedema is swelling of deeper tissues (skin, mucosa) due to increased vascular permeability.
Mechanistic types:
Histaminergic (allergic) responsive to antihistamines, steroids, epinephrine.
Bradykinin-mediated (e.g. hereditary, ACE-inhibitor induced) requires targeted therapies (C1-INH, icatibant, etc.).
Triggers: Foods, medications, insect stings, contrast agents, trauma, drugs (especially ACE inhibitors)
Diagnosis: Clinical history, complement and C1-INH testing, allergy workup
Treatment: Depends on cause
For histaminergic: antihistamines, steroids, epinephrine
For bradykinin-mediated: C1-INH, icatibant, supportive care
Always secure the airway in severe cases
Prevention: Avoid known triggers, monitor and adjust medications, prophylactic therapy where indicated
Cephalexin capsules distributors: In pharmaceutical trade, various companies supply cephalexin capsules. If you are looking for distributors in your area, I can assist.
If you like, I can prepare a version of this write up tailored to a specific audience (patients, medical students, healthcare professionals) or localize it for India (with guidelines) or even provide a list of cephalexin distributors in Gujarat or your city. Would you like me to do that?